 Azoospermia is the medical condition of a male not having any measurable level of sperm in his semen. It is associated with very low levels of fertility or even sterility, but many forms are amenable to medical treatment. In humans, azoospermia affects about 1% of the male population and may be seen in up to 20% of male infertility situations. Azoospermia is the medical condition of a male not having any measurable level of sperm in his semen. It is associated with very low levels of fertility or even sterility, but many forms are amenable to medical treatment. In humans, azoospermia affects about 1% of the male population and may be seen in up to 20% of male infertility situations.
Classification : Azoospermia can be classified into three major types as listed. Many conditions listed may also cause various degrees of oligospermia rather than azoospermia.
Pretesticular azoospermia : Pretesticular azospermia is characterized by inadequate stimulation of otherwise normal testicles and genital tract. Typically, follicle-stimulating hormone (FSH) levels are low (hypogonadotropic) commensurate with inadequate stimulation of the testes to produce sperm. Examples include hypopituitarism (for various causes), hyperprolactinemia, and exogenous FSH suppression bytestosterone. Chemotherapy may suppress spermatogenesis. Pretesticular azoospermia is seen in about 2% of azoospermia .
Testicular azoospermia : In this situation the testes are abnormal, atrophic, or absent, and sperm production severely disturbed to absent. FSH levels tend to be elevated (hypergonadotropic) as the feedback loop is interrupted. The condition is seen in 49-93% of men with azoospermia.Testicular failure includes absence of failure production as well as low production and maturation arrest during the process of spermatogenesis.
Causes for testicular failure : include congenital issues such as in certain genetic conditions (e.g. Klinefelter syndrome), some cases of cryptorchidism or Sertoli cell-only syndrome as well as acquired conditions by infection (orchitis), surgery (trauma, cancer), radiation,or other causes. Mast cells releasing inflammatory mediators appear to directly suppress sperm motility in a potentially reversible manner, and may be a common pathophysiological mechanism for many causes leading to inflammation. Generally, men with unexplained hypergonadotropic azoospermia need to undergo a chromosomal evaluation.
Posttesticular azoospermia : In posttesticular azoospermia sperm are produced but not ejaculated, a condition that affects 7-51% of azoospermic men.The main cause is a physical obstruction (obstructive azoospermia) of the posttesticular genital tracts. The most common reason is a vasectomy done to induce contraceptive sterility.Other obstructions can be congenital (example agenesis of the vas deferens as seen in certain cases of cystic fibrosis) or acquired, such as ejaculatory duct obstruction for instance by infection.
Ejaculatory disorders : include retrograde ejaculation and anejaculation; in these conditions sperm are produced but not expelled.
AYURVEDIC TREATMENT: There is no satisfactory treatment of azoospermia in allopathic treatment system hence ayurvedic treatment is most preferred treatment for this condition. The treatment involves both medicinal treatment as well as panchkarma treatment for the same.
Medicinal Treatment: Various herbs are known for their effects in increasing the sperm count of the patients e.g. Musli sufed, Munjatak, Makkhan, Ashwagandha, Shatavari, etc. Along with the herbs there are various classical combinations which are very helpful for treating this condition like Makardhwaj wati, Suwarna Siddha Makardhwaj, Shilajeet Adi wati, etc.
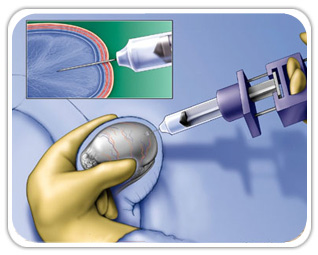
Ayurvedic Panchkarma therapies:A special panchkarma procedure known as Uttar basti is very helpful for this condition, Uttar basti should be given under the supervision of a trained ayurvedic doctor only.
|



{kind=link}
 (0)9831775590
Book appointment
(0)9831775590
Book appointment